
From Pilot to National Infrastructure: What 58+ NHS Trusts & Health Boards Reveal About Radiology AI at Scale
By Dr Mark Phillips, Chief Clinical Officer at Harrison.ai
Dianne had a persistent cough1. Her GP had a low index of suspicion for cancer, something just didn’t feel quite right, and sent her for a chest X-ray.
The image was busy. There were a few chronic findings, and a very subtle area of increased opacification that, on most days, might have prompted a “probably nothing, come back in six weeks just to be sure” follow-up. This time, the AI zoomed in on it. Dianne had a same-day CT, a biopsy two weeks later, and a resection a few weeks after that. She was diagnosed with Stage 1 primary lung cancer. She is now all clear.
That is the whole story, told plainly. A subtle shadow, a busy X-ray, an AI that flagged it immediately, and a cancer caught at the stage where it can still be cured.
But here is what makes Dianne’s story important: it is not exceptional. That is precisely the point.
Across more than 58 NHS Trusts and Health Boards, the tools that highlighted Dianne’s cancer are now in routine use. This is the story of how that happened, and what it took to get there.
A system under structural pressure
Healthcare systems face serious pressure as demand for diagnostic imaging surges while clinical capacity remains constrained. This shortage creates backlogs and delays critical findings, leaving radiologists overwhelmed, processing hundreds of scans daily while subtle details can be missed. Training a radiologist takes more than a decade and imaging volumes keep climbing. The gap between the two is where patients wait. And it continues to widen.
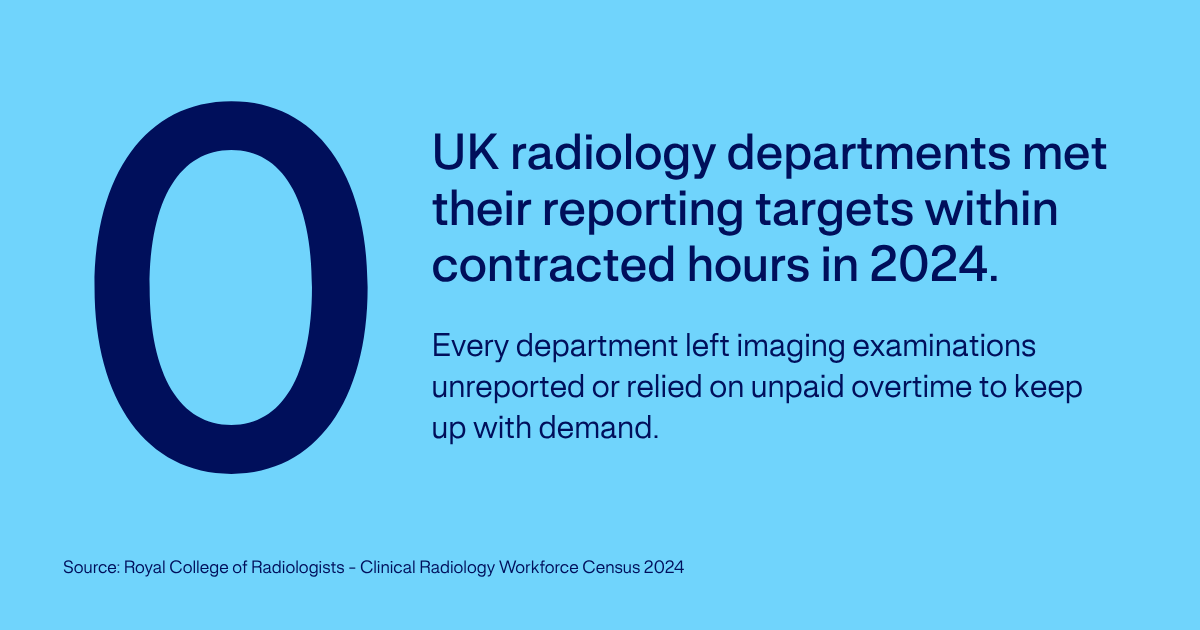
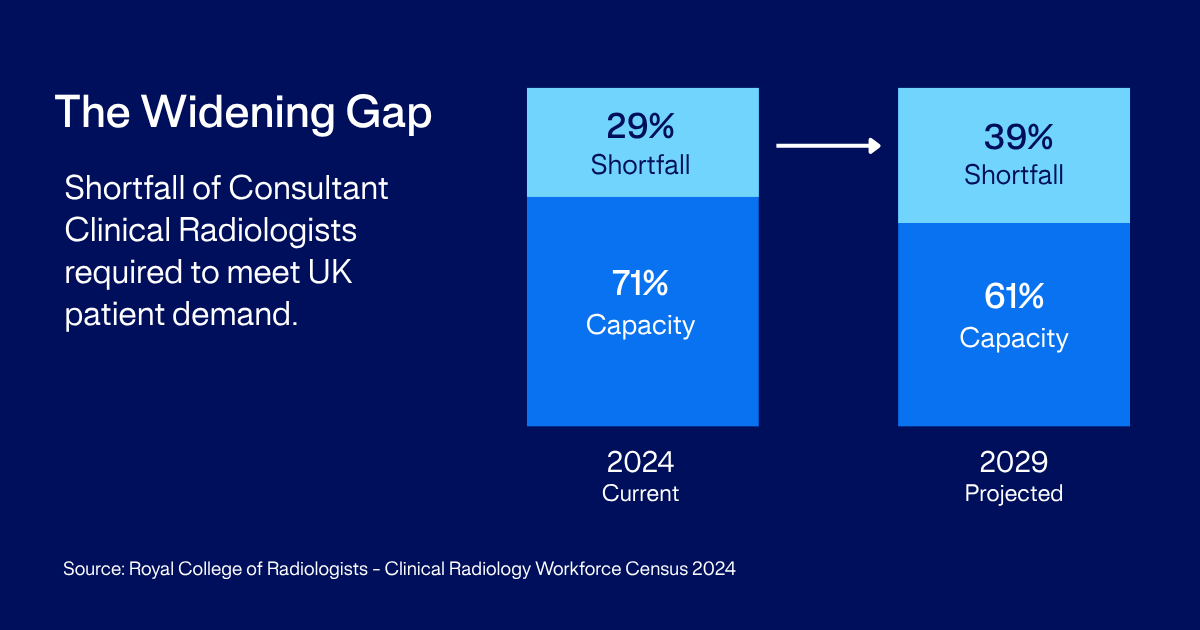
The numbers are stark. Globally, there is an average of ~45 radiologists per million population.2 Even in well-resourced health systems, this has proven insufficient: in the UK alone, the workforce of consultant clinical radiologists is currently short by 29%, a shortfall forecast to rise to 39% by 2029 if no action is taken.3 In the NHS, the backlog of unread imaging studies has been a persistent feature of the system for years. For the first time in 2024, not a single radiology department in the UK could meet its reporting requirements within staff contracted hours. All were leaving imaging examinations unreported or relying on unpaid overtime.3
Radiologists are not failing to work hard enough. Demand for CT and MRI imaging grew by 8% in 2024, while the radiology workforce grew by just 4.7%, causing vital diagnostic services to fall further behind.4 They are working in a system that structurally cannot keep pace with demand.
The clinical consequences of that pressure are not abstract. The AIDE study, a recent Australian retrospective study, re-analysed the imaging histories of patients later diagnosed with lung cancer. Harrison.ai Chest X-ray (CXR) identified a suspected lung nodule on a chest X-ray from 2015, reported at the time as not suggestive of lung cancer, and again on a scan two years earlier still.5 The AI found what the system, under pressure, had not flagged. This is not a criticism of the radiologists who read those scans. The pattern is not unique to one health system; it is what comprehensive AI does in any system under pressure – a second set of eyes that does not tire, does not carry the cognitive load of the previous 200 imaging examinations, and does not miss the subtle.
“AI is extremely helpful in identifying subtle abnormalities that might be missed by my heavy workload.”
Anonymous NHS clinician, post-implementation survey
The radiologists and clinicians doing extraordinary work under structural pressure to keep this system running deserve tools that match the scale of what they are being asked to do. That is what AI is for.
From pilot to national infrastructure
There is a threshold in any technology deployment where it stops being a pilot and starts being infrastructure. Harrison.ai’s NHS deployment has crossed that threshold.
More than 58 NHS Trusts and Health Boards encompassing 150+ hospitals now have the technology live and in clinical use – representing approximately 40% of the NHS.6
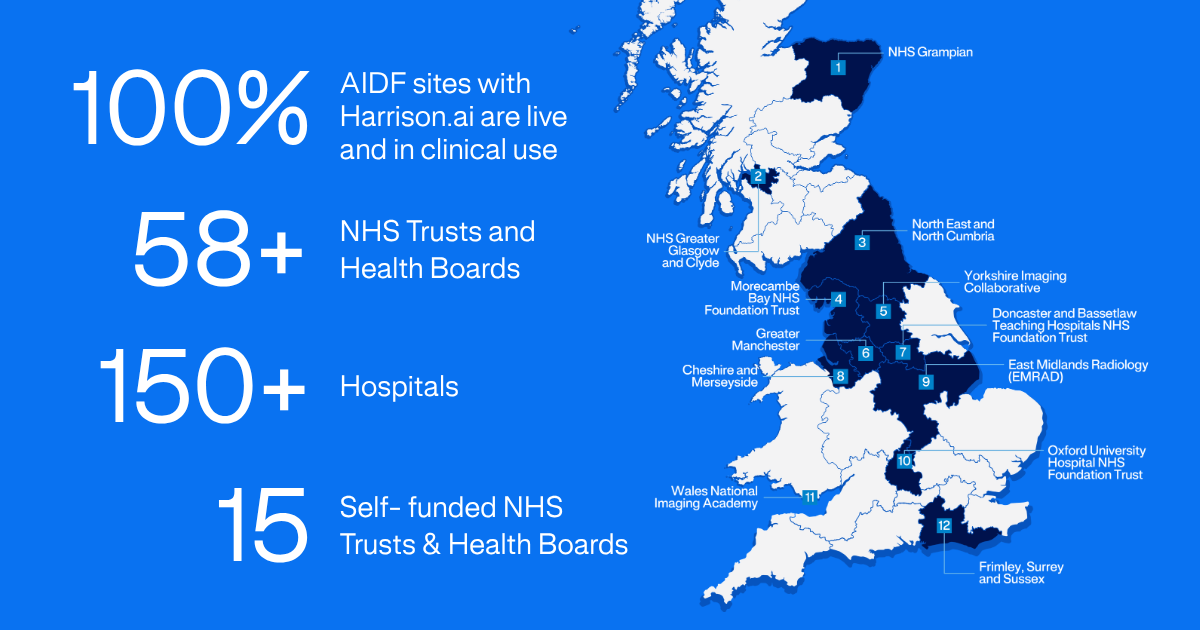
The path to that scale was not without difficulty. In 2023, the AI Diagnostic Fund, an award-winning £21 million NHS England programme to accelerate AI adoption in diagnostic imaging, placed its trust in Harrison.ai CXR across six imaging networks: Cheshire and Merseyside, East Midlands, Greater Manchester, North East and North Cumbria, Frimley-Sussex-Surrey, and Yorkshire. First-of-kind deployments at this scale required more evidence, more clinical champion investment, and more time than anyone anticipated. 100% of AIDF sites with Harrison.ai are now live and in clinical use, many for over a year – work recognised by the Prime Minister’s AI Exemplar Award.

Tom Pickersgill, Regional Director UK & Ireland, at 10 Downing Street to present the NHS AI Diagnostic Fund results to Prime Minister Keir Starmer.
The rigour of NHS clinical safety governance is not a constraint on deployment. It is the standard that any technology operating at national scale should be held to. And one that Harrison.ai was built to meet.
What the evidence shows
Reimagining the lung cancer pathway
Lung cancer is one of Scotland’s most common cancers and remains the leading cause of cancer death in the country. NHS Grampian deployed Harrison.ai CXR as part of its lung cancer diagnostic pathway. The results were significant: the proportion of patients diagnosed and treated within the 62-day target moved from 52% to 100%.7 Every patient. 100% of lung nodules were detected earlier.
Unlocking economic value
The clinical case for AI is well established. The economic case is less often articulated clearly. Two years into NHS AI Diagnostic Fund deployment, the operational data is starting to give us some of the clearest numbers yet.
Out-of-hours CT brain scans, those taken overnight or at weekends, are typically sent to external teleradiology providers at a per-scan cost. At Doncaster and Bassetlaw Teaching Hospitals NHS Foundation Trust, AI-assisted triage now identifies which scans can safely wait for the in-house radiology team in the morning and which cannot. The annual cost saving from that change is in the order of £134,4008, once AI-assisted triage carries its share of overnight reads. But the case at Doncaster does not stop at radiology. Around 20% of Emergency Department CT brain patients become eligible for earlier discharge because they are no longer waiting on an overnight read.8 A workflow change becomes a flow-of-patients change.
That is worth pausing on. The same workflow change registers in two places at once: money saved on overnight radiology, and patients becoming eligible to leave hospital sooner. Repeated across the NHS, that points toward savings reinvested in care, fewer patients sitting waiting on results, and a capacity gap finally beginning to narrow.
Finding what you were not looking for
The Christie NHS Foundation Trust is one of Europe’s leading cancer centres. Their deployment of Harrison.ai CXR produced a finding that goes to the heart of why comprehensiveness matters clinically. In a retrospective review of 955 lateral chest X-rays in their cancer patient population, AI-assisted interpretation produced a 39% increase in vertebral fragility fracture detection9 compared with standard reporting, fractures that carry serious implications for quality of life in patients who have survived their cancer. Early detection accelerates intervention and reduces the risk of future complications, which have a significant cost impact to the NHS.
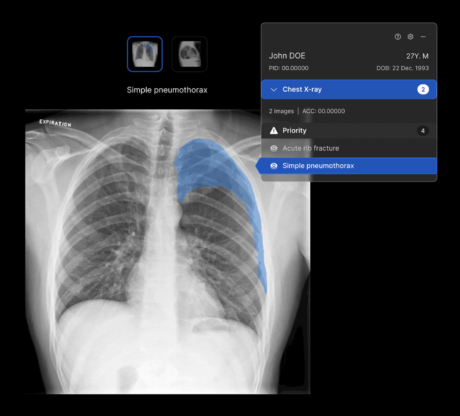
This is what comprehensive AI detection means in practice. A radiologist reading a chest X-ray for a known clinical question is cognitively focused on that question. Harrison.ai CXR reads the whole image against all 124 radiological features it has been trained to detect. That comprehensiveness is not a product feature, it is a clinical safety argument.
Explore how AI could drive clinical and operational benefits for your organisation.
What clinicians and NHS Trusts are choosing
The truest measure of clinical value is an NHS Trust choosing to pay for something out of its own budget.
Across the NHS, Trusts that deployed Harrison.ai through the AIDF programme are now choosing to self-fund continued access. That decision, made under real budget pressure, is the strongest signal of clinical value.
“This advanced solution helps by intelligently prioritising the reporting worklist, ensuring patients with abnormal findings are identified quickly and moved through the pathway without delay. We are pleased that the Trust has decided to continue using Harrison.ai beyond the initial year, reinforcing our dedication to adopting innovative technologies that enhance patient care.”
Mike Jones, Radiology AI/Digital Lead and Advanced Practitioner Radiographer (Chest)
Royal Surrey NHS Foundation Trust
Where this goes next
The NHS deployment is not the end of this story, it is the proof of concept the rest of the world is watching. Harrison.ai is clinically deployed across every public Emergency Department in Hong Kong, alongside approximately half of Australia’s radiologists, with active deployments in 21 countries. Each of those deployments is generating its own evidence. What is distinctive about the NHS is the diversity inside it: 58+ Trusts and Health Boards, 150+ hospitals, multiple clinical settings, all operating independently. That is the closest any health system has come to a national-scale, real-world test of what comprehensive AI does in routine practice. The findings will matter everywhere.
What no one yet knows is what a national health system actually looks like after a decade of comprehensive AI running across it. How much capacity gets freed up. What it saves the system. How many patient outcomes change. The NHS is one of the first health systems in a position to tell us.
What is already clear is what changed for Dianne – a subtle, early-stage cancer caught because the clinician was supported by the right tools. That’s the answer that already matters.
Dr Mark Phillips is Chief Clinical Officer at Harrison.ai where he leads the clinical strategy ensuring the company’s radiology AI is safe, evidence-based and genuinely useful to the care teams who rely on it.

See it for yourself
Explore how AI could drive clinical and operational benefits for your organisation.
References
- BBC – AI cancer diagnosis ‘might have saved my life’
- RCR 2024 Clinical Radiology Workforce Census Report
- RCR Staff shortages are a ticking time bomb for cancer patients
- AIDE study (HREC 101791)
- Data on file
- Realistic Medicine: Taking Care, Chief Medical Officer for Scotland Annual Report 2023–2024
- Data on file
- Presented by Frost, F., WCO-IOF-ESCEO (2025) Rome, Italy